
Gastrointestinal mastocytosis carries risks even when symptoms are missing
Even without symptoms, gastrointestinal mastocytosis carries a risk of bone marrow involvement, according to new research.
Even without symptoms, gastrointestinal mastocytosis carries a risk of bone marrow involvement, according to new research.

People with SM may require significantly higher doses of adrenaline and early admission to intensive care when experiencing anaphylaxis.

Patients with SM experience higher frequencies of multisystem symptoms both in the year before and after diagnosis.

Conventional tryptase thresholds (~11 μg/L) should be maintained rather than raised, and tryptase alone is insufficient to rule out SM.

Researchers found CD123 expression in 91% of SM cases, showing it is a frequent and stable marker in nearly all disease subtypes.

In addition to serum tryptase, urinary biomarkers may be a useful tool in identifying and managing SM, research review concludes.
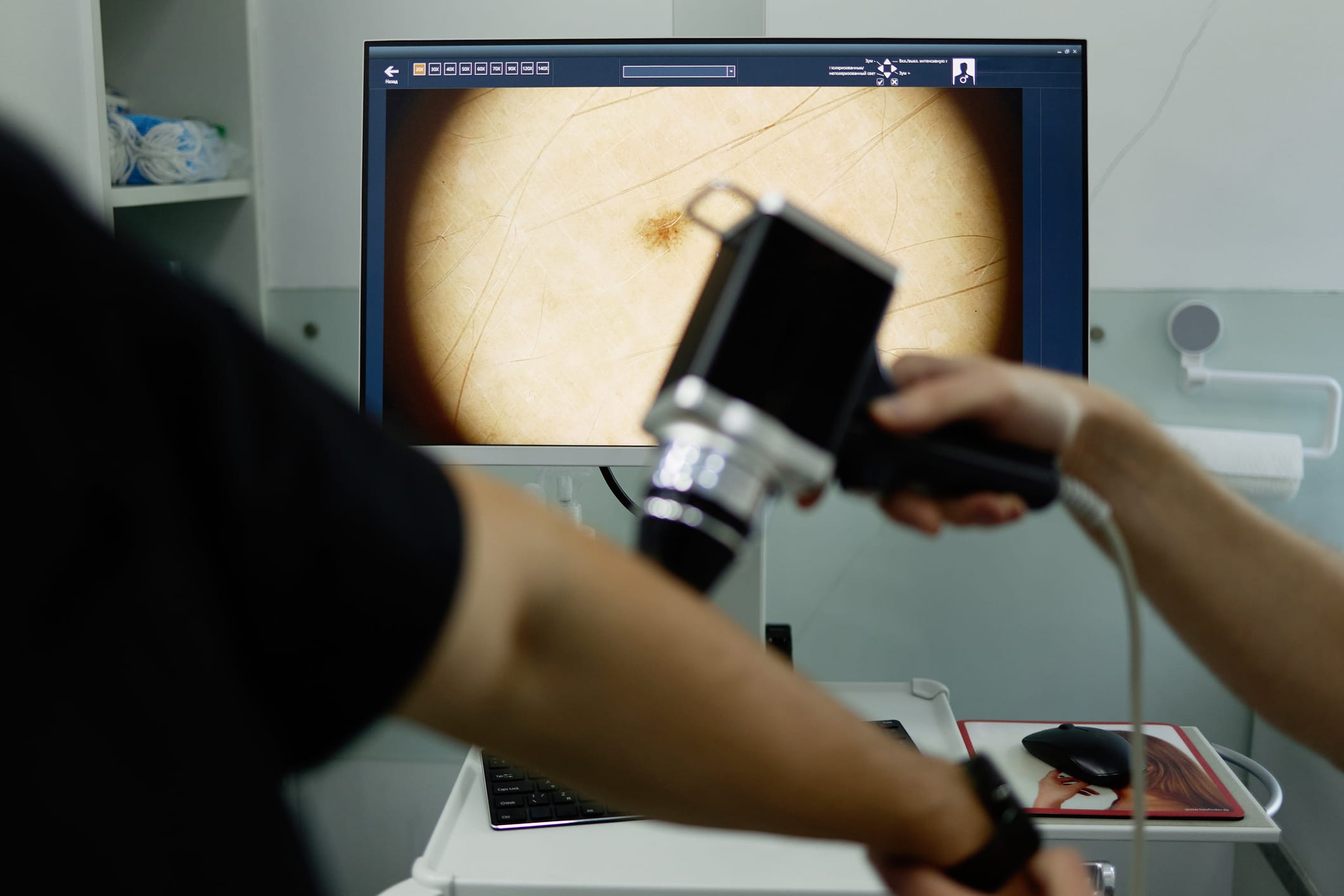
A 67-year-old man with returning melanoma was found to have SM after genetic testing on his tumor showed unusual results.

ST2, a receptor that binds with interleukin-33, is elevated in patients with SM and may be a biomarker and future therapeutic target.
The application is supported by results from the SUMMIT trial. A decision is expected by December 30, 2026.

Peg-interferon-alfa2a (peg-IFN-α) offers a promising approach for treating bone disease in non-advanced systemic mastocytosis.

